This may appear to be yet another disagreeable whinge from a slightly opinionated FST but if a favourable outcome is to be had from surgical interventions the anaesthetist has to have the equipment and medication to do the job and similarly the surgeon has to have the equipment that he needs.
We requested a diathermy apparatus. Basically this is a large transformer which generates a high frequency spark and is used by the surgeon to stop bleeding whilst he is cutting tissue. It cauterises the wound and speeds up the procedure and shortens operating time.
In the absence of a blood bank it was vital that as little blood as possible was lost and it is obvious that speed is critical.
The absence of either of these aids reduces safety and impairs efficiency. The absence of both compounds the problem.
On the anaesthetic side the lack of nitrous oxide, limited supply of oxygen and neostigmine meant that anaesthetic techniques had to be used from which the patients recovered more slowly.
This is actually quite important. If someone is unconscious and unable to protect their own airway they need an attendant; one person out of the thirteen FST members until their consciousness improves.
The absence of a mechanical ventilator meant that when a patient had to have a muscle relaxing anaesthetic the anaesthetist had to ventilate him for the duration of the operation by squeezing a black rubber bag or pumping a bellows up and down as well as engaging in all the other vital tasks to keep him alive. Ventilators run on either compressed gas or electricity. The Manley ventilator provided ran on compressed gas and we had only a very small amount of that to use in an emergency.
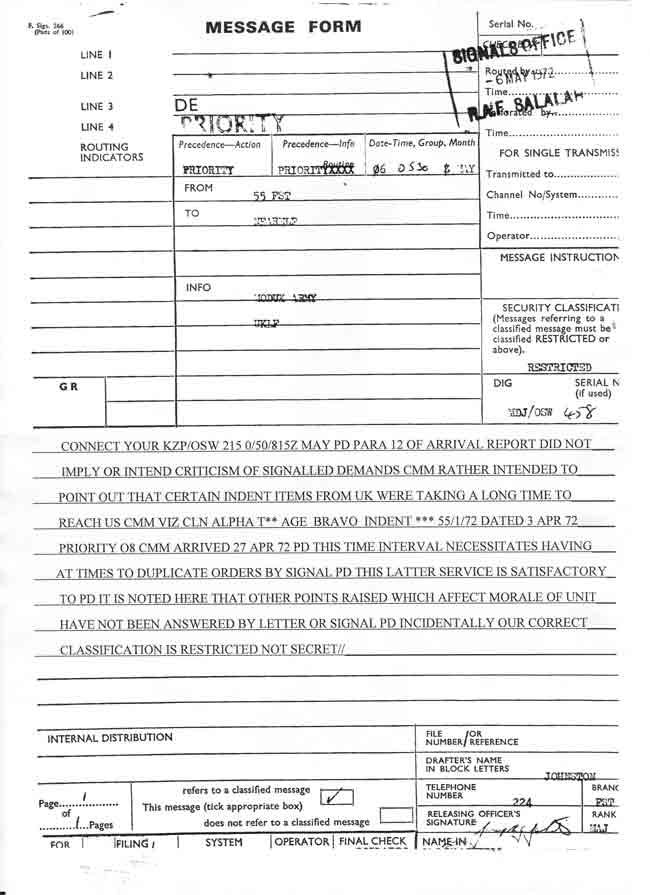
Diathermy, blood bank,anaesthetic kit could have been dispatched from Ludgershall and been on site in Salalah in 72 hours.
We were not whingeing without a fully justifiable reason.
Ludgershall did provide a diathermy machine eventually, about half way through our tour. They did NOT however provide the electrodes to connect it to the patient……
The Resupply Scandal
This may appear to be yet another disagreeable whinge from a slightly opinionated FST but if a favourable outcome is to be had from surgical interventions the anaesthetist has to have the equipment and medication to do the job and similarly the surgeon has to have the equipment that he needs.
We requested a diathermy apparatus. Basically this is a large transformer which generates a high frequency spark and is used by the surgeon to stop bleeding whilst he is cutting tissue. It cauterises the wound and speeds up the procedure and shortens operating time.
In the absence of a blood bank it was vital that as little blood as possible was lost and it is obvious that speed is critical.
The absence of either of these aids reduces safety and impairs efficiency. The absence of both compounds the problem.
On the anaesthetic side the lack of nitrous oxide, limited supply of oxygen and neostigmine meant that anaesthetic techniques had to be used from which the patients recovered more slowly.
This is actually quite important. If someone is unconscious and unable to protect their own airway they need an attendant; one person out of the thirteen FST members until their consciousness improves.
The absence of a mechanical ventilator meant that when a patient had to have a muscle relaxing anaesthetic the anaesthetist had to ventilate him for the duration of the operation by squeezing a black rubber bag or pumping a bellows up and down as well as engaging in all the other vital tasks to keep him alive. Ventilators run on either compressed gas or electricity. The Manley ventilator provided ran on compressed gas and we had only a very small amount of that to use in an emergency.
Diathermy, blood bank,anaesthetic kit could have been dispatched from Ludgershall and been on site in Salalah in 72 hours.
We were not whingeing without a fully justifiable reason.
Ludgershall did provide a diathermy machine eventually, about half way through our tour. They did not however provide the electrodes to connect it to the patient……