Anaesthesia
That piece of cutting edge anaesthetic equipment shown above was what we had in BMH Rinteln in the early 70’s. Perhaps at a time when anaesthesia had developed more into a science than being a rather arcane art.
One of the preferred anaesthetic techniques at the time, because it gave a good outlook for the patient and ideal operating conditions for the surgeon, was endotracheal intubation, paralysis and positive pressure artificial ventilation.
What more could a surgeon ask of his anaesthetist ?
Practically a bit of kit like the Boyles Machine shown above needs bottles of high pressure specialist gases – nitrous oxide, oxygen cyclopropane etc etc. It needs them at the rate of perhaps 8 litres per minute. That is the equivalent of two cylinders per hour or the same weight as two 25pdr shells; possibly a logistic challenge if the FST were busy. It may need CO2 absorption granules too, in closed circuit, to remove carbon dioxide. The gas may also be needed to power a ventilator. Additional kit to measure other parameters in the paralysed patient is needed; blood pressure monitors, pulse meters etc etc
Providing the surgeon with what he demands – surgeons demand they don’t just want – is not too difficult a task if you are on the end of a logistic supply line and in a brick built building on the north German plain.
Not so in Dhofar.
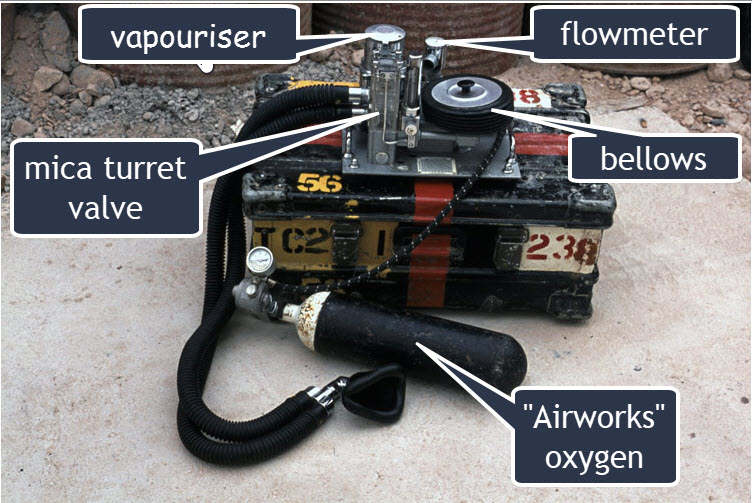
The anaesthetic apparatus that was available in RAF Salalah was a flexible one devised by Major General Stephens in the 1960’s – The Haloxaire. It was for use where there were limited resources . This was a device which could be used for simple draw over anaesthesia- air or gases were sucked through a vapouriser by the patient and the fumes sent him to sleep. Alternatively the patient could be paralysed and intubated and the anaesthetic vapours forced into his chest with rubber Oxford bellows regulated by a series of mica discs in a turret device. It was manufactured by a company named Cyprane from Yorkshire who are no longer trading.
Anaesthetic Agents
The drug used to keep the patient asleep and anaesthetised was halothane. This pungent liquid was evaporated in a temperature compensated vapouriser which gave accurate control of the percentage of anaesthetic delivered. Halothane was and is a slightly tricky drug to use as it can cause cardiac irregularities. At least it is not explosive like ether.
So far so good. We have used a gas – air – to deliver our anaesthetic agent to the patient.
Our next move is to paralyse the patient and artificially ventilate his or her lungs.
Ventilation
The core of the Haloxaire is a Perspex turret with some discs of mica inside that function as valves. Cleverly designed, this allows tha patient to breathe either spontaneously and normally or, with the aid of the bellows, to be artificially ventilated by the anaesthetist. The amount of air being ventilated through the patient is measured with a Wrights flowmeter.
Ancillary Devices
Blood pressure can be measured with a simple cuff, pulse with finger to the wrist, oxygen saturation by seeing if the patients lips are blue. Muscle relaxation by complains from the surgeon that the abdomen is rigid or by your own feeling that the lungs are resisting ventilation. It is in these seemingly peripheral essential that experience is essential.
We have, with a minimum of equipment, provided in a dusty “F” Section tent a reasonable approximation of the anaesthetic conditions that would satisfy even a fussy surgeon.
Crude anaesthesia such as this is labour intensive – try ventilating a thirteen stone Fijian by hand for two hours. All sorts of other things go on during an anaesthetic such as the monitoring of vital signs and the top ups of the drugs used in the process, the administration of fluids or blood down to the simple essential task of keeping the surgeon amused by telling him what you, the anaesthetist, think are funny stories.
The procedure needs both an anaesthetist and an Operating Theatre Technician (ODP as they are now known as) who are experienced.
This is simple robust equipment with very little to go wrong and no batteries to go flat that is driven by the man rather than the man depending on complex electronic gizmos which will take any opportunity to leave him in the lurch.It is a question of equipping the man rather than manning the equipment.
The concept of simple reliable anaesthetic equipment was further developed as in the Tri-Service Anaesthetic Equipment by Brigadier Ivan Houghton L/RAMC. His apparatus required only a couple of small tins of anaesthetic agents and not the two “25pdr” equivalents per hour of the more common base hospital anaesthetic techniques.
It is interesting to note from a title on one of David Raitt’s photographs “who needs nitrous oxide” that even by 1976 it appears that no up to date anaesthetic machine had been provided and the trusty Haloxaire, with a bit of oxygen from Airworks, was still in use.