A MONTHS HOLIDAY IN THE SUN
1976 was the summer of the great drought. At the end of the summer we took the children with our caravan to West Wales for a holiday between Milford Haven and Dale. It poured with rain for 10 days. So disgruntled were we with the weather that we packed up early and drove home late on the Friday, arriving back in Stubbington in the early hours of Saturday morning. The children were tired and miserable, Anne was tired and miserable and I was tired and miserable. As usual when we arrived home after being away for any length of time there was a mountain of mail on the doorstep which I gathered up and took into the dining room and dumped on the table. I then put the kettle on for a cup of tea while Anne put the children to bed.
While we were having tea, we sorted through the mail and I was intrigued to see a letter from the Director of Naval Surgery. It was from JR[1] and read,
“I am writing to ask if you would be prepared to spend a month’s holiday in Salalah…”
Anne was not amused,
“I suppose that’s in the sun !” she muttered. And so it was.
The first question on my mind was, of course, what am I supposed to be doing there, and in this respect JR was unhelpful but he did suggest that I went up to London to see Surgeon Commander Alan McEwen, who was then the officers’ appointer. (He was also known as “The Colonel” for reasons that became all too obvious.) He would be able to give me the information I required. And so I made an appointment to see him and fell in to his office in Empress State Building in Earls Court. I knocked on his door,
“Who are you and what do you want?” I told him and added, “I have an appointment.”
“Now you’re going where?” he asked. I thought as the appointer he should know.
“Salalah.” I said. “I want to know why I am going and what am I supposed to do when I get there.”
“Bear with me, “ He said, “I’ll ring a chum.” With that he put his feet up on the desk and took hold of the phone. There was a rather flamboyant conversation with his chum.
“Hello, it’s Alan here. I’ve got a fellow with me who has been seconded out to Salalah. What can you tell me about it?”
There were lots of “Yes”, “No”, “Really” and “Good heavens” and he finished the conversation,
“…well thanks for all that. Must meet for a gin some time. Chin, chin.”
He replaced the phone and turned to me.
“Well,” he said, “I can’t tell you anything about what’s expected of you, but I can tell you that its f***ing hot out there.” And that was the end of the interview.
I think that my fear of flying started with the flight to Oman. I went by Gulf Airlines from Heathrow to Oman via Bahrain and Abu Dhabi. It was an horrific flight, punctuated by hours of clear air turbulence, sitting on the ground in Abu Dhabi for hours with no air conditioning and finally landing in Muscat with, as we came in to land, a wing commander sitting next to me grabbing hold of the seat in front of him and shouting,
“What the hell is he doing?”
If he was upset and he knew about flying how should I feel?
At Muscat, I was taken away by an elderly major, who gave me a beer. It was his job to get me to Salalah and I had a choice. There was an Iranian Hercules going almost immediately or if I preferred, in a couple of hours there would be a Sultan of Oman’s Air Force BAC111 also going. I opted for the BAC111. It was an uneventful flight over thousands of square miles of uninhabited desert on which the only landmarks were the oil wells. There were also only seven of us on an aeroplane capable of taking two hundred.

SOAF BAC 111 at the new Runway in Salalah
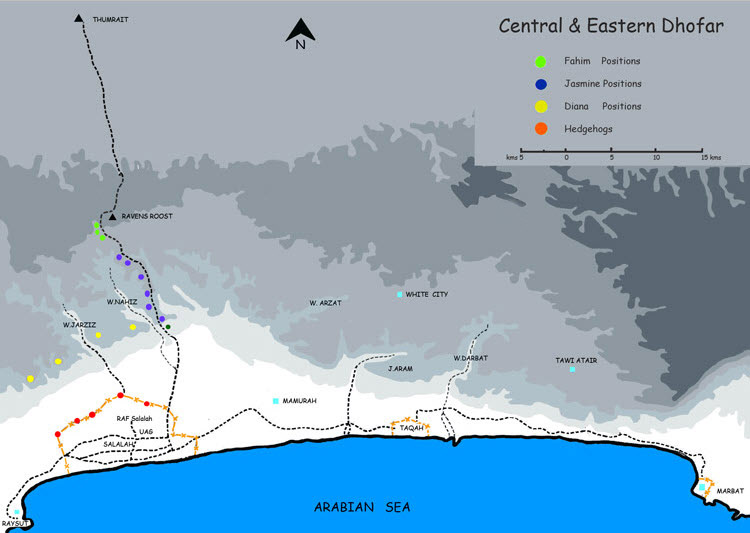
Salalah was a small town about 50Km from the border with the South Yemen. RAF Salalah was in the Dhofar province of Oman. The base was run by the RAF but housed the HQ Dhofar Brigade of the Sultan’s Armed Forces and the HQ of the Sultan of Oman’s Air force. In 1976, there was an Army Field Surgical Team, (FST) operating from the base, and the incumbent surgeon, Colonel Bob Scott, had to fly home and since neither the Army nor the RAF had anyone with the required experience available, I had been summoned to deputised for him – the first Royal Navy surgeon to be appointed to this front line post.
As usual I had a comprehensive briefing and handover. When I climbed out of the aeroplane at Salalah there was a figure at the bottom of the ladder already holding a suitcase.
“Hello” He said, “I’m Bob Scott. It’s all yours. Bye……”[2]
And with that he climbed the ladder and disappeared.
There had been a protracted war in Oman for some years. In 1970, the present Sultan, Quaboos bin Said took over from his Father in a bloodless coup. On the accession of the new ruler, there were many social and political changes in the country, including the abolition of slavery and the use of money accrued from the sale of oil for the encouragement of industry and the provision of modern medical and educational services. Not everybody agreed with the changes and the antiroyalists were Marxist forces, trained in the Communist Bloc and infiltrated into the country from the Peoples Republic of the South Yemen. The terrorists were known locally as the Adoo. By 1976 the Adoo had effectively been defeated but they were still active and their legacy remained with occasional terrorist incursions into the Djebel Mountains and the presence of thousands of square miles of minefields, to a large extent uncharted. Indeed, they were still being laid by the Adoo.
The FST was there to look after battle casualties incurred as a result of isolated skirmishes between the Sultan’s Forces and the Yemenis and antipersonnel mine injuries and to cater for the medical requirements of the RAF Base personnel and to act as a private medical facility for UK contract civilians and any Omani civilians, who preferred to attend the FST rather than go to their own doctors. So far as the Sultan’s Armed Forces were concerned, they were for the most part led by contract officers, retired British Army officers. They insisted on the provision of modern medical facilities if they were shot or injured and hence the FST. The Sultan knew that if he dispensed with the FST then most of his contract officers would walk off the hill.
55 FST Salalah – A Soldier’s welcome for a Sailor!
The FST was made up of a small complex of buildings within the base. Next to the FST was a helicopter where casualties could be landed. The mortuary was a refrigerated container which was usually used for keeping the beer cool. The team itself was made up of myself as the surgeon, a physician who was also the anaesthetist called Colonel Don Hutton, and a dental officer, Squadron Leader David Clements who doubled as the second anaesthetist. There were additionally, 13 other ranks from the Army and RAF who made up the nurses and technicians.
The equipment was the standard equipment used by all Service mobile surgical teams although because the FST had been established for some years the equipment had been augmented to make life more comfortable from the clinical standpoint.
The only commodity not freely available was blood. This was “On the hoof”. If blood was required for a major casualty, the requirement was broadcast on Radio 219, the local British radio station which was operated from within the base. All the ex-patriot British listened to the station and our experience was that within 10 minutes of broadcasting a need for a particular blood group there would be a queue of donors outside the FST.
From the morning after my arrival, helicopters arrived regularly with casualties of one sort or another. We always knew when casualties were inbound because on the wall of the compound in which we lived there was a huge alarm bell. When this bell sounded helicopters were about 5 minutes away – just time enough to run over to the FST to meet them. We all developed a Pavlovian reaction to bells and my conditioning did not wear off for months after I got back.
The first patients to arrive within minutes of starting work were from a road traffic accident (RTA). One was dead, one had a serious head injury and the third appeared uninjured but decided that having been brought down from the mountains he might as well go into town to do some shopping and meet his pals! This phenomenon was very common and meant that any Omani casualty, brought down from the Djebel was usually accompanied by his whole family.
RTAs were extremely common because Omanis were the worst drivers in the World. Most common among the accidents were those caused by cornering too fast, usually with a trailer on the back of a lorry. In one incident, however, a land rover driving down a dead straight road collided with a petrol tanker coming in the opposite direction in a remote part of the desert about 350 Km north of Salalah. They were the only two vehicles on the road at the time. We got the petrol tanker driver about 6 hours after the accident and he was suffering from 90% burns. Unfortunately and not surprisingly, he died.
The Iranians were in Oman in great numbers and their main base was at Thumrait, in the mountains. They regularly exercised with the Omani Army and their Hercules aircraft regularly landed at Salalah. Landed is probably something of a euphemism for what actually occurred because the stories of the exploits of Iranian pilots at take off, landing and indeed in the air became legion. But as they say in the Fleet Air Arm,
“If you walk away from it, it counts as a landing.”
Thank goodness I was not persuaded to fly down to Salalah in one of their aeroplanes the first time I arrived in Oman. They had apparently written off at least half of their fleet of aircraft during their time in Oman.
They were also less than disciplined with their military hardware. We had a constant stream of Iranian casualties through the FST, ranging from a couple of squaddies suffering from burns, who had been smoking in an oxygen store, to gun shot wounds. One of the most serious incidents involved a sergeant and his corporal. The corporal had had a negligent discharge from his weapon, had shot himself through the thumb, but more importantly had shot his sergeant through the right forearm. This resulted in the first of many amputations that I had to carry out during this trip, and resulted in some very unpleasant interviews with senior Iranian Army officers, who always wanted to hold an inquest into the patient’s treatment, usually by the patient’s bedside.
The Arab population appeared to be ambivalent to life and death, so much so that we had to be careful that it did not rub off on to us. Just outside the FST was a patio, covered by a parachute. It was here that we would relax in the shade. On the patio was a loofah tree and in the tree lived a chameleon called Henry who was very tame and would eat tit-bits out of our hands. One day casualties were due by helicopter, and as was customary the base fire engines arrived to stand by the pad whilst the helicopters were landing and taking off. Henry was crossing the road and was run over. He was picked up by our “Matron”, a short fair haired cockney Army nurse. He rushed over to me and said,
“Look at Henry, Boss.”
I examined the beast who had had his tail and back legs crushed. There was nothing I could do for him so I said to Matron,
“Go and put him out of his misery.”
A few minutes later he came back.
“I’ve put Henry to sleep, Boss.”
“What did you use, ether or chloroform?”
“Neither, I took him round the back and beat his brains out with a brick.”
A dangerous attitude ambivalence!
My duties were not confined to the FST. I discovered that I was also the visiting “consultant” to the Um al Guarif Military Hospital in Salalah, to which I was taken by chauffeur driven Limousine once a week to conduct a ward round. I actually enjoyed these excursions because I did enjoy teaching and the SHOs running the hospital were certainly keen to learn. I struck up a very good working relationship with Col Mehdi, the CO of the hospital which resulted in being invited round to his house, shortly before we left for a curry supper cooked by his wife – probably the best curry meal I have ever had either before or since.
We also went, about once a fortnight into downtown Salalah where we conducted an outpatient clinic at a local dispensary. This enabled the local British contingent to obtain British medical advice rather than having to rely on the local civilian doctors, most of whom were either Indian or Pakistani. Fortunately most of the Brits were healthy and if anything did crop up that needed treatment we normally insisted that they go back to the UK for treatment. I did, however, reluctantly carry out some vasectomies – at a price.
Salalah was not exactly the social capital of the Middle East and many of the population working there were ex-patriots, many from the UK, but others from Greece, India and Pakistan. So we made our own evening entertainment. For us it was easy, if nothing was happening we simply went to the mess and for very little money, had wonderful food and ice cold beer. We were however often invited out and we spent many very enjoyable evenings with the folk at Taylor Woodrow having barbeques, with the Greek engineers who were building the new Salalah Airport eating unspeakable Greek food, washed down with neat whisky, gin or vodka, and often we were invited to the homes of local notables in the medical profession. The most hair-raising night was when I was asked to be the guest at Trafalgar Night at Airworks Mess.
Airworks was a British company on contract to service all the SOAF aircraft. It was made up for the most part by ex Fleet Air Arm Engineer Senior Ratings and when they celebrated, they did so in style. I got dressed up in full mess undress and went over to their mess. They too had dressed for the occasion, many in their old RN uniforms. The first event of the evening was, “Up Spirits”. A coffin[3] was ceremonially brought into the mess and placed in front of the President. He opened it and produced a case of Navy rum. This was mixed 1:1 with water and then everybody had a tot. I had to have the first, and one in the middle and the last – and I hate the stuff. Everybody kept drinking the rum until it was gone. Then we had a meal.
Now I have only vague memories of the remainder of the evening. I do remember standing in one of the quadrangles outside the mess, hanging on to a pillar because it was the only thing I could find that was not rotating! At some stage later in the evening I decided I had had enough and wanted to go home and somebody offered to take me back to my basha which was right across the other side of the airfield, in a land rover. Half way over the airfield I decided I wanted a pee so I got out of the land rover, at about 40 mph. I was extraordinarily lucky in that I only twisted my ankle but it could have been considerably worse. I felt very sorry for myself for several days.
Many of the civilian patients who arrived at the FST had been sent down from the mountains by the British Army Training Team (BATT) who spent most of their time in the Djebel carrying out hearts and minds duties in return for intelligence on active terrorists. Part of their humanitarian task was to obtain medical aid for the tribesmen. I was approached one day and asked if I would go up to the Djebel and see some patients that they wanted advice about. The first problem was to get properly equipped so I was issued with a proper set of combat clothing, a pair of Dhofar boots, which are green suede combat boots, (Which I still have to this day), an M16 Armalight rifle, 100 rounds of ammunition and three spare magazines.
“Hang on,” I thought.
I was taken up to the Djebel in a Defender. These were Brittan Norman Islander propeller driven aircraft, built in the Isle of Wight which were perfect to use as air taxis because they were small, light, could carry up to 6 passengers at a time and could land on short grass air strips. The pilots were all retired RAF pilots and in spite of the official end to the hostilities, they were still attacked by surface to air missiles and small arms fire from time to time and were therefore very watchful when flying into the mountains. Their standard procedure was to fly at about 8000 feet until they were over the location where they were to land, they would then stand on one wing and spiral down, flattening out to land. Nobody told me about this manoeuvre until we were airborne, and for somebody who hates flying at the best of times I found this terrifying. Particularly so when on landing there was a crashed aircraft at the end of the grass strip, and, as I later discovered, the mountain tribesmen were using the body of another crashed aircraft as a home. They must have been used to passengers throwing up on landing because nobody turned a hair. At least I got out of the aircraft first.
The Djebel was very beautiful because it was shortly after the Harif, or monsoon, and everywhere was very lush and green. In many ways it resembled the Lake District, although I was assured that this would not last long, and the hillsides would soon be scorched brown by the intense heat of the sun. My primary job was to assist the BATT on their rounds, see patients and advise on their treatment.
A standard day would involve leaving our camp, visiting outlying villages, where the BATT would help the villagers in any way they could, transporting water supplies, treating the sick and wounded, and acting as taxis. They had quite a comprehensive medical kit, and on one occasion I actually pulled a tooth, which was more difficult than I expected but very satisfying for the patient once the pus from his dental abscess had been released. Wherever we went we were greeted warmly, invited to drink very sweet herbal tea or thick sweet coffee. As soon as they heard there was a doctor in the village, the queue formed stretching over the horizon. Once seen we were always sent on our way with fresh fruit and vegetables, including fresh sweet corn, and cucumbers that looked like marrows.
A Well Dressed Surgeon on the Djebel
It was in these villages that I came across another demonstration of the ambivalence towards life and death. Children with diarrhoea and vomiting were very common and we saw countless children, dehydrated, comatose and clearly near death. I saw about 4 or 5 baby girls in this state and although the parents were quite young, they refused all our attempts to treat the babies citing, “Insh’allah” or “It is God’s will” whether they lived or died. They were, however, very insistent that we treat all the boys in the same state even if that meant, as it usually did, flying them down to the civilian hospital in Salalah.
I returned to Salalah after a week in the mountains to find that it had been very quiet at the FST but that all changed within 24 hours.
On the Sunday we were invited to Sunday Lunch at the HQ of the Frontier Force at Raysut by their Medical Officer Captain Dipu Ganguli. The Officers’ Mess was in a wonderful position high on a cliff overlooking the sea. From the patio outside the bar, you could look over the wall straight down into the sea and see turtles swimming at the base of the cliff in the crystal clear, light blue water. We had a curry lunch and a few beers with the Second in Command, (We will call him Peter) and his officers and then left to allow them to get some sleep because they were going on an operation near the border that night. We said our farewells and returned to Salalah.
At 2300 that night, the bell rang and a helicopter arrived with a staff sergeant from the Frontier Force who had stepped on an anti-personnel mine. When he arrived he was deeply shocked and had clearly lost an enormous amount of blood. He was still bleeding profusely from several sites and we decided to break all the rules of resuscitation by anaesthetising him so we could stem the haemorrhage. This we did. I then set about the task of debriding his wounds and tidying up his left leg from which his foot had disappeared. We finished operating at 0400 and went to bed.
At 0630 the bell rang again, and I arrived at the FST at the same time as the helicopter. Dipu Ganguli was holding a drip for a patient on a stretcher. I met him at the edge of the helipad,
“Hello John,” He said, “It’s Peter and I think he’s dead.”
Peter had led a rescue the night before to recover the staff sergeant and in investigating the mine site at dawn, had himself trodden on an anti-personnel mine about 20 metres from where his staff sergeant had been blown up.
This officer was in serious trouble
The first thing we needed was blood and so we rang Radio 219. The bad news was that his blood group was ‘O’ Negative. Remarkably within 10 minutes we were bleeding donors. Try as we might we could not get his blood pressure up and we were clearly losing the battle. For the second time in 24 hours we had to dispense with conventional wisdom and anaesthetise him in order to resuscitate him. Under anaesthetic I removed what remained of his right leg, applied pressure bandages to his other limbs, then went off for a cup of coffee while my anaesthetic colleagues, Don Hutton and David Clements continued the resuscitation. I realistically thought that I would not be required any further. I was wrong.
After about half an hour, Don Hutton came into the coffee room and said,
“He’s as good as we can get him, now it’s up to you.”
I don’t think I have ever felt such responsibility before, or indeed since. I began a seven hour operation which was remarkable for all the wrong reasons. Not the least was the necessity not to allow this opportunity to pass without taking photographs. I operated with a camera always to hand and those photographs were, and still are very valuable. I was carrying out surgery that I had only ever read about in books and there was nobody there to offer advice, tutelage or criticism. We held the life of a British Army officer in our hands in a Nissen hut in the middle of the desert.
Even then the black humour of the medical and nursing professions came to the fore and in some way kept us all sane. To relieve the tension, I asked for some music in the background while we were operating and one of the nursing staff scurried away to get their ghetto blaster. Most of the time we had easy listening pops and classics, until somebody asked,
“Any requests ?”
As if we had all been telepathically linked the answer came back,
“How about Andy Fairweather Lowe – Wide Eyed and Legless.”
From that moment we all knew that our patient was going to survive.
The operation itself was relatively simple. All his wounds were debrided, cleaned and packed with antiseptic swabs. The haemorrhage was arrested. Although he clearly had penetrating injuries to both his eyes, I had no experience of ophthalmic surgery and no operating microscope so I put antibiotics into both eyes and padded them.
All foreign bodies were excised and removed. This was especially important in his left leg. When we turned him over and began to work on his left leg, he had two large wounds in his buttock. I inserted my finger into one of the wounds and felt a foreign body which, when I removed it turned out to be the heel from his combat boot.
In all we operated on Peter for 7 hours. He received 17 pints of blood beside other intravenous fluids and at the end of the operation was in remarkably good shape considering his injuries. He was sent back to the ward for intensive nursing.
We were clearly not going to be able to look after this patient for any length of time and he needed the expertise of a major injuries unit. We got hold of the Base Operations Officer and told him that this man and his staff sergeant needed urgent airlift to the UK and 24 hours later he was on his way back to the Queen Mary Hospital at Roehampton, where he made a full recovery.
There is a sequel to this story. In 1978 I was the surgeon at the Royal Naval Hospital in Gibraltar and I met a Royal Marine Officer who had also served in Oman. We talked, as you do, about old times and he mentioned a friend of his, Peter, who had been seriously injured in Oman. It was the same Peter. My Royal Marine friend suggested that when we got back from Gibraltar, he would have a party and invite Peter and myself, so that we could meet. I actually forgot about this conversation until late in 1979, an invitation arrived in the post from the Royal Marine, to go to a party at his house near Chichester.
Anne and I drove over to Chichester on the appointed night, but having arrived outside the house, I suddenly had cold feet about going inside and meeting Peter again. Anne was adamant,
“We’ve come this far, there’s no going back.”
So in we went. We were met at the door by Penny, who was evidently Peter’s wife. She ushered us into a room where there was a group of people talking, including a man with a false leg and a patch over one eye. As the conversation progressed somebody asked,
“What do you do for a living, John ?”
“I’m a surgeon in the Navy.” I replied.
At this, our friend turned to me and said,
“You’re a surgeon in the Navy. Do you know somebody called John Soul ?”
“That’s me.” I said.
“My God,” he said, “We’ve met before.”
“Yes for an hour or two a few years ago.”
He grabbed me by the arm.
“My Dear Chap,” He said quietly, “I think I owe you a beer.”
We then spent a large part of the evening reminiscing – as you do.
There was a further sequel to this story. I was at a Livery Dinner at the Society of Apothecaries in London some months later and sat opposite a pathologist who happened to work at Roehampton. The conversation inevitably led to discussing the casualties who came back from Oman and he knew all about Peter.
“What a pity you didn’t get any photos.” He said. “We would have been interested to see them.” Of course I did, and so did they.
I was invited to Roehampton later in the year to give an account of our exploits in Oman and when I arrived at the hospital lecture theatre it was packed to the doors. I was introduced and stood up and delivered my lecture for about forty minutes. The latter part of the lecture involved the pictures of Peter on admission and during the course of his surgery and I described in great detail how we had resuscitated him and all the surgery we had carried out. At the conclusion of the lecture there was muted applause and I was asked if I would take any questions. A distinguished figure in the front row got up and addressed the audience,
“I was the duty consultant the night that Peter was brought in to us,” he began, “And when I examined him, I could not believe the barbarity of the surgery that had been performed on this unfortunate patient.” He then turned to me and said,
“Having seen the pictures you took when he was admitted to you and during the course of the surgery I can only say how wrong I was to have misjudged completely both the extent of his initial injuries and the lengths to which you went to save this man’s life. How you ever got him back to us alive I will never know.”
The answer was, of course, that was our job. We were a team and a good one at that and in that team we all played our part. On this occasion we all got it right.
At the end of October we were relieved in Salalah by a surgical team from the RAF. We had the usual round of “Ma’Salaam” or farewell parties and eventually climbed on board an RAF VC10 bound for Brize Norton in Oxfordshire where we were reunited with our families. At the time it was extraordinary, that on the basis of a months experience in the desert, and having operated on about 6 major casualties, I was the most up to date and experienced surgeon in the Royal Navy on the treatment of high velocity missile wounds and anti-personnel mine injuries. It seemed to me then, and the opinion is still valid that unless we give our surgeons and anaesthetists this sort of experience at every available opportunity, the service we provide to our customers in the operational role we support will always be second best and that is not good enough.[4]
[1] Surgeon Commander John Richardson FRCS – Director of Naval Surgery
[2] Bob Scott was found dead in the sea off his yacht off Dartmouth two years later.
[3] The “Tot” had been abolished in 1970/71 and many old sailors still to this day mourn its passing.
[4] Since 1976 the Royal Naval Medical Service has conspicuously been involved in the Falklands Iraq and Afghanistan. My concern no longer applies.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.